 AI
AI
 AWS
AWS
 Agile
Agile
 Algorithms
Algorithms
 Android
Android
 Apple
Apple
 Bash
Bash
 C++
C++
 Csharp
Csharp
Content
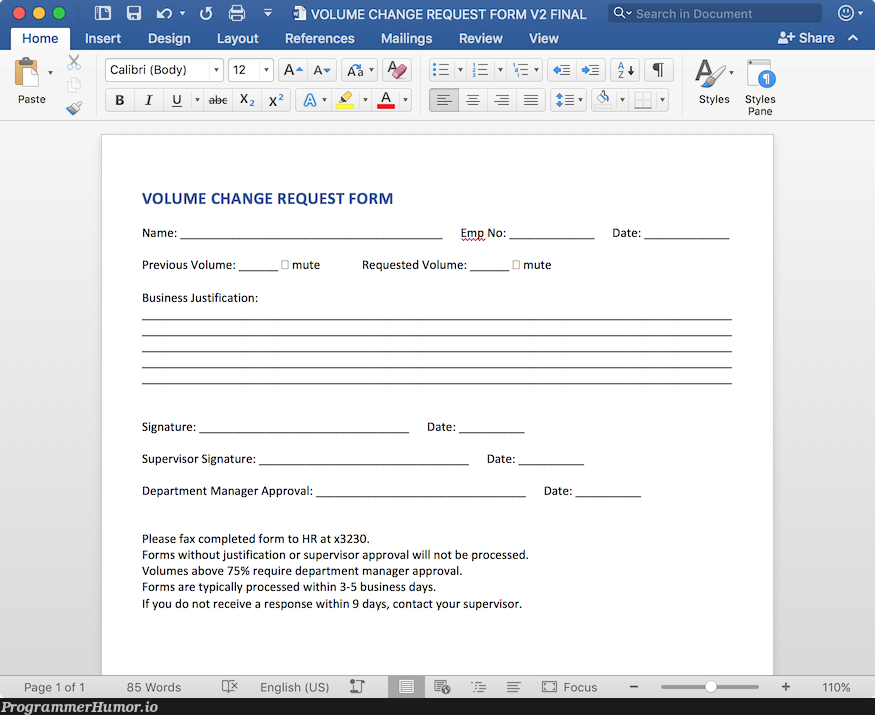
Home Insert Pasto Design Calibri (Body) I 8 Layout 12 r a0 x2 VOLUME CHANGE REQUEST FORM V2 FINAL References Mailings Review View Q Search in Document As Av Aa v A EVE A A Stvles Share Styles Pang VOLUME CHANGE REQUEST FORM Name: Previous Volume: mute Business Justification: Emp No: Date: Requested Volume: O mute Signature: Supervisor Signature: Department Manager Approval: Date: Date: Date: Please fax completed form to HR at x3230. Forms without justification or supervisor approval will not be processed. Volumes above 75 require department manager approval. Forms are typically processed within 3-5 business days. If you do not receive a response within 9 days, contact your supervisor. Page 1 of 1 85 Words English (US) E Focus 110